TB – Gold Quantiferon:
Why TB - Gold QuantiferonTest ?
CLINICAL INFORMATION
Tuberculosis is a contagious disease that usually targets the lungs. Tuberculosis is caused by Mycobacterium tuberculosis (MTB).
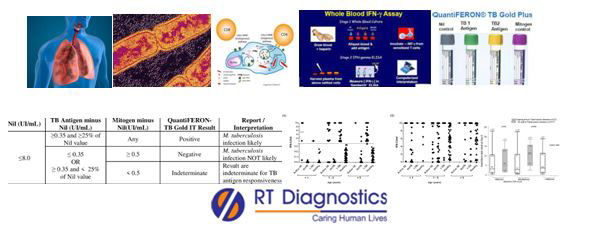
AFB – Acid Fast Bacillus is a kind of bacteria that is the causative agent for tuberculosis (TB).Tuberculosis is a serious bacterial infection that mainly affects the lungs and can be spread from person to person (communicable disease) through coughing and sneezing (minute tiny droplets). The infection begins when the mycobacteria reach the alveolar air sac of the lungs. The mycobacterium tuberculi bacteria are identified as foreign and are thus phagocytosis occurs. During this process, the mycobacterium tuberculi are enveloped by the macrophage and are stored in a membrane-bound vesicle called a phagosome. These phagosomes combine with lysosomes to form phago-lysosome. Thus these phago-lysosomes use reactive-oxygen species and acids to kill these mycobacterium tuberculi. As the mycolic acid present in the capsule of Mycobacterium tuberculosis, it protects from these toxic substances. Meanwhile, these bacteria then invade those endosomes of alveolar macrophages and replicate. Therefore they reproduce inside the macrophage and kill the immune cell. The primary site of infection in the lungs is known as the Simon focus (if found in the top of the lung) or Ghon focus (if located in the upper part of the lower lobe). Tuberculosis is classified as one of the granulomatous inflammatory diseases. Macrophages, epithelioid cells, T Lymphocytes, B Lymphocytes and fibroblasts aggregate to form granulomas, with the lymphocytes surrounding the infected macrophages. These infected macrophages are attacked by other macrophages to form giant multinucleated cells in the alveolar lumen. These granulomas prevent the dissemination of mycobacteria. Two forms of TB are latent TB and active TB. Latent TB is described when the body’s immune system prevents the infection from spreading (formation of granulomas where the TB is confined within granulomatous tissue as a tubercle where necrosis occurs at the centre – resulting in caseous necrosis and heals by fibrosis) and the clinical manifestations are masked. Active TB is a pathological state where the bacteria becomes active. Three stages of TB are the initial phase - exposure (impact after initial contact), latent phase, and active disease (dissemination with extra-pulmonary manifestations eg. brain, kidney, spine etc). Notable extrapulmonary infection sites include the pleura (in tuberculous pleurisy), CNS (tuberculous meningitis), lymphatic system (scrofula of the neck), the genito-urinary system (urogenital tuberculosis), bones and joints (Pott disease of the spine), potentially widespread form of TB is military or disseminated TB. Moreover from the primary site of infection which is the lungs, reactivation can spread to other parts of the body (disseminated tuberculosis or military tuberculosis) such as brain, spine and kidneys (extra-pulmonary TB)etc.AFBsmear for mycobacteria is performed in laboratory on specimen samples such as sputum, phlegm etc. Clinical manifestations upon initial exposure include fever, weakness, weight loss, night sweats, respiratory symptoms (like upper respiratory tract manifestation) may be mild or can persist for many months etc. Other signs and symptoms include intense lower respiratory tract manifestations of lung disease such as nasal congestion, coughing, blood-stained sputum, phlegm, coughing out of blood, enlarged lymph nodes, bone or joint pain, persistent headache, confusion, seizures etc. High-risk factors include smokers, immuno-compromised patients, patients with impaired immune systems, patients with immunosuppressive drugs, undernourished or malnourished people, healthcare workers in hospitals (a nosocomial infection that is resistant strains eg. multidrug-resistant TB), diabetes mellitus, genetic susceptibility etc. Prevention for TB can be achieved by BCG immunization. Complete medical evaluation for TB (Tuberculosis), must include a medical history, a physical examination, a chest X-Ray and microbiological examination (eg. Sputum specimen) moreover it may also include supporting tests like BACTEC, tuberculin or Mantoux skin test, scans like CT, X-Rays, interferon-gamma release assays, and MMR (Abreugraphy) and surgical biopsy. Associated tests include alternative sampling, PCR, FDG PET/CT, immunological tests, Trans Dermal Patch Assay, Heaf test, ADA test, NAAT, LAM Detection Assays, and other confirmatory tests on the clinical sample (sputum, pus, tissue biopsy) specimen analysis for TB are conducted etc. The Quantiferon-TB Gold test (QFT-G) is a highly specific and sensitive analytical method with strong predictive diagnostic tests for patients with true infection of M.tuberculosis. QFT is a whole blood test that helps in detecting Mycobacterium tuberculosis infection, latent tuberculosis infection, tuberculosis (TB) disease etc. QFT is an interferon-gamma (IFN-gamma) release assay also known as IGRA. The principle of this test is that when suspected patients’ WBCs when are infected with M. tuberculosis will release interferon-gamma (IFN-g) when mixed with antigens, the immune response is, evident and hence tests result is declared positive. The disadvantage of this method is that it cannot differentiate between active tuberculosis and latent tuberculosis infection and hence this test result is intended for use with risk assessment (clinical evaluation), radiography and application of other medical and diagnostic interpretations. Therefore, clinical skills with experience can analyze and extrapolate precise judgment. Nowadays more recent advancements (such as tuberculin skin test, PPD, and Mantoux test is used to diagnose latent tuberculosis infection) with evidence-based treatment have brought about a scientific revolution (CD8+ AND T cell Technology etc provides a more comprehensive picture of patients’ immune response against TB) in medical research for enabling more accurate assessment (eg. cell-mediated response to TB infection).
Additional tests include tuberculin or Mantoux skin test, BACTEC, scans like CT, X-Rays, interferon-gamma release assays and MMR (Abreugraphy) and surgical biopsy. Other tests include other confirmatory tests on the clinical sample (sputum, pus, tissue biopsy) specimen analysis for TB are conducted, alternative sampling, PCR, FDG PET/CT, immunological tests, Trans Dermal Patch Assay, Heaf test, ADA test, NAAT, LAM Detection Assays etc.
General Instructions:
Sample Requirement: Specimen - Blood sample collected from the vein. Test Preparation: None.
NOTE - Sample for specimen collections may vary based on the patient’s condition/cases according to the patient’s presenting complaints/signs or symptoms:
SPECIMEN REQUIREMENT (Special or Rare Cases) - As instructed and guided by Physician / Clinician / Pathologist / as per Laboratory’s requirements, according to procedures and protocols.
This Multi-Specialty Clinical Referral Laboratory RT DIAGNOSTICS provides precise and accurate tests with an extensive range of testing services to the medical centres to help in the diagnosis and identification of pathology in the test specimens for infectious diseases and also to evaluate the function of organ systems of the patient. It prevents further complications and helps to stabilize and restore health to near normalcy at the earliest without delay.